Coronary arteries of the heart
In this section, you will become familiar with the anatomical arrangement of the coronary vessels of the heart. To get acquainted with the anatomy and physiology of the cardiovascular system, you should visit the section "Heart Diseases".
- Left coronary artery.
- Right coronary artery
The blood supply to the heart is carried out through two main vessels - the right and left coronary arteries, starting from the aorta immediately above the semilunar valves.
Left coronary artery.
The left coronary artery begins from the left posterior sinus of Vilsalva, goes down to the anterior longitudinal sulcus, leaving the pulmonary artery to the right of itself, and to the left - the left atrium and the ear surrounded by fatty tissue, which usually covers it. It is a wide, but short trunk, usually no more than 10-11 mm in length.
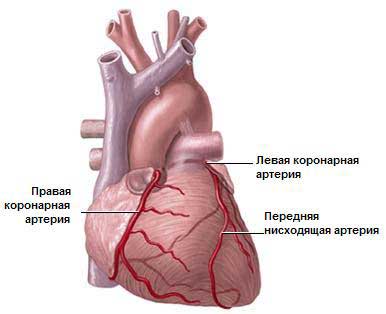
The left coronary artery is divided into two, three, in rare cases into four arteries, of which greatest value for pathology have anterior descending (LAD) and circumflex branches (OB), or arteries.
The anterior descending artery is a direct continuation of the left coronary artery.
Along the anterior longitudinal cardiac groove, it goes to the apex of the heart, usually reaches it, sometimes bends over it and passes to the posterior surface of the heart.
Several smaller lateral branches depart from the descending artery at an acute angle, which are directed along the anterior surface of the left ventricle and can reach the blunt edge; in addition, numerous septal branches depart from it, piercing the myocardium and branching into the anterior 2/3 of the interventricular septum. The lateral branches feed the anterior wall of the left ventricle and give branches to the anterior papillary muscle of the left ventricle. The superior septal artery gives rise to a branch to the anterior wall of the right ventricle and sometimes to the anterior papillary muscle of the right ventricle.
Throughout its entire length, the anterior descending branch lies on the myocardium, sometimes plunging into it with the formation of muscle bridges 1-2 cm long. For the rest, its anterior surface is covered with epicardial fatty tissue.
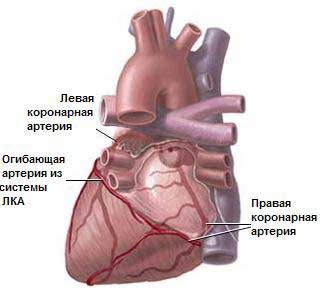
The enveloping branch of the left coronary artery usually departs from the latter at the very beginning (the first 0.5-2 cm) at an angle close to a straight line, passes in the transverse groove, reaches the blunt edge of the heart, bends around it, passes to the posterior wall of the left ventricle, sometimes reaches the posterior interventricular sulcus and in the form of the posterior descending artery is directed to the apex. Numerous branches extend from it to the anterior and posterior papillary muscles, the anterior and posterior walls of the left ventricle. One of the arteries supplying the sinoauricular node also departs from it.
Right coronary artery.
The right coronary artery begins in the anterior sinus of the Vilsalva. First, it is located deep in the adipose tissue to the right of the pulmonary artery, bends around the heart along the right atrioventricular groove, passes to the posterior wall, reaches the posterior longitudinal groove, and then descends in the form of a posterior descending branch to the apex of the heart.
The artery gives 1-2 branches to the anterior wall of the right ventricle, partly to the anterior septum, both papillary muscles of the right ventricle, posterior wall of the right ventricle and posterior interventricular septum; the second branch also departs from it to the sinoauricular node.
There are three main types of myocardial blood supply: middle, left and right. This subdivision is based mainly on variations in the blood supply to the posterior or diaphragmatic surface of the heart, since the blood supply to the anterior and lateral regions is fairly stable and not subject to significant deviations.
At middle type all three main coronary arteries are well developed and fairly evenly developed. The entire left ventricle is supplied with blood, including both papillary muscles, and the anterior 1/2 and 2/3 of the interventricular septum, through the system of the left coronary artery. The right ventricle, including both right papillary muscles and the posterior 1 / 2-1 / 3 septum, receives blood from the right coronary artery. This appears to be the most common type of blood supply to the heart.
At left type blood supply to the entire left ventricle and, in addition, the entire septum and partially the posterior wall of the right ventricle is carried out due to the developed enveloping branch of the left coronary artery, which reaches the posterior longitudinal sulcus and ends here in the form of the posterior descending artery, giving away part of the branches to the posterior surface of the right ventricle ...
Right type observed with a weak development of the circumflex branch, which either ends without reaching the obtuse edge, or passes into the coronary artery of the obtuse edge, without extending to the posterior surface of the left ventricle. In such cases, the right coronary artery, after branching of the posterior descending artery, usually gives off several more branches to the posterior wall of the left ventricle. In this case, the entire right ventricle, the posterior wall of the left ventricle, the posterior left papillary muscle and partially the apex of the heart receive blood from the right coronary arteriole.
The blood supply to the myocardium is carried out directly :
a) capillaries lying between the muscle fibers, braiding them and receiving blood from the coronary artery system through the arterioles;
b) a rich network of myocardial sinusoids;
c) the vessels of Viessant-Tebezia.
As the pressure in the coronary arteries increases and the work of the heart increases, blood flow in the coronary arteries increases. Lack of oxygen also leads to a sharp increase in coronary blood flow. Sympathetic and parasympathetic nerves, apparently, have little effect on the coronary arteries, exerting their main effect directly on the heart muscle.
Outflow occurs through veins collecting in the coronary sinus.
Venous blood in the coronary system is collected in large vessels, usually located near the coronary arteries. Some of them merge, forming a large venous canal - the coronary sinus, which runs along the posterior surface of the heart in the groove between the atria and ventricles and opens into the right atrium.
Intercoronary anastomoses play an important role in coronary circulation, especially in pathological conditions. There are more anastomoses in the hearts of people suffering from ischemic disease, therefore, the closure of one of the coronary arteries is not always accompanied by necrosis in the myocardium.
In normal hearts, anastomoses are found only in 10-20% of cases, with a small diameter. However, their number and magnitude increase not only in coronary atherosclerosis, but also in valvular heart disease. Age and gender by themselves do not have any effect on the presence and degree of development of anastomoses.
Heart (cor)
The circulatory system consists of a huge number of elastic vessels of various structures and sizes - arteries, capillaries, veins. At the center of the circulatory system is the heart, a living, pressure-and-suction pump.
The structure of the heart. The heart is the central apparatus of the vascular system, highly capable of automatic action. In humans, it is located in the chest behind the sternum, for the most part (2/3) in the left half.
The heart lies (Fig. 222) on the tendon center of the diaphragm almost horizontally, located between the lungs in the anterior mediastinum. It occupies an oblique position and is turned by its wide part (base) upward, backward and to the right, and by its narrower cone-shaped part (top) forward, downward and left. The upper border of the heart is in the second intercostal space; the right border protrudes approximately 2 cm beyond the right edge of the sternum; the left border passes, not reaching the mid-clavicular line (passing through the nipple in men) by 1 cm. The apex of the heart cone (the junction of the right and left contour lines of the heart) is placed in the fifth left intercostal space down from the nipple. In this place, at the time of contraction of the heart, a heart beat is felt.
Rice. 222. The position of the heart and lungs. 1 - heart in a cordial shirt; 2 - diaphragm; 3 - tendon center of the diaphragm; 4 - thymus gland; 5 - lung; 6 - liver; 7 - sickle ligament; 8 - stomach; 9 - unnamed artery; 10 - subclavian artery; 11 - common carotid arteries; 12 - thyroid gland; 13 - thyroid cartilage; 14 - superior vena cava
In shape (Fig. 223), the heart resembles a cone, with its base facing upwards and its top facing downwards. Large blood vessels enter and exit the wide part of the heart - the base. Heart weight in healthy adults ranges from 250 to 350 g (0.4-0.5% of body weight). By the age of 16, the weight of the heart increases 11 times compared with the weight of the heart of a newborn (V.P. Vorobiev). Average dimensions of the heart: length 13 cm, width 10 cm, thickness (anteroposterior diameter) 7-8 cm. In terms of volume, the heart is approximately equal to the clenched fist of the person to whom it belongs. Of all vertebrates, birds have the largest relative heart size, which needs a particularly powerful motor to move blood.
Rice. 223. Heart (front view). 1 - unnamed artery; 2 - superior vena cava; 3 - ascending aorta; 4 - coronary groove with the right coronary artery; 5 - right ear; 6 - right atrium; 7 - right ventricle; 8 - apex of the heart; 9 - left ventricle; 10 - anterior longitudinal groove; 11 - left ear; 12 - left pulmonary veins; 13 - pulmonary artery; 14 - aortic arch; 15 - left subclavian artery; 16 - left common carotid artery
In higher animals and man, the heart is four-chambered, that is, it consists of four cavities — two atria and two ventricles; its walls consist of three layers. The most powerful and most important functionally is the muscle layer - the myocardium. The muscle tissue of the heart is different from the skeletal muscle; it also has a transverse striation, but the ratio of cellular fibers is different than in the muscles of the skeleton. The muscle bundles of the heart muscle have a very complex arrangement (Fig. 224). In the walls of the ventricles, it is possible to trace three muscle layers: the outer longitudinal, the middle annular and the inner longitudinal. There are transition fibers between the layers, which constitute the predominant mass. The outer longitudinal fibers, deepening obliquely, gradually pass into annular, which also obliquely gradually pass into the inner longitudinal; from the latter, the papillary muscles of the valves are formed. On the very surface of the ventricles, there are fibers that cover both ventricles together. Such a complex course of muscle bundles provides the most complete contraction and emptying of the heart cavities. The muscular layer of the walls of the ventricles, especially in the left, which drives blood in a large circle, is much thicker. The muscle fibers that form the walls of the ventricles, from the inside, are collected in numerous bundles, which are located in different directions, forming fleshy beams (trabeculae) and muscle protrusions - papillary muscles; tendon cords run from them to the free edge of the valves, which stretch with the contraction of the ventricles and do not allow the valves to open under the pressure of blood in the atrial cavity.
Rice. 224. The course of the muscle fibers of the heart (semi-schematic)
The muscular layer of the atrial walls is thin, since they also have a small load - they only drive blood into the ventricles. The superficial muscle pikes, facing the inside of the atrial cavity, form the comb muscles.
From the outer surface on the heart (Fig. 225, 226), two grooves are noticeable: a longitudinal one, covering the heart in front and back, and a transverse (coronal), located annularly; along them are the own arteries and veins of the heart. These grooves correspond to septa inside, dividing the heart into four cavities. The longitudinal interatrial and interventricular septum divides the heart into two completely isolated from each other half - the right and left heart. The transverse septum divides each of these halves into the upper chamber - the atrium (atrium) and the lower - the ventricle (ventriculus). Thus, two non-communicating atria and two separate ventricles are obtained. The superior vena cava, inferior vena cava and coronary sinus flow into the right atrium; the pulmonary artery departs from the right ventricle. The right and left pulmonary veins flow into the left atrium; the aorta departs from the left ventricle.
Rice. 225. Heart and large vessels (front view). 1 - left common carotid artery; 2 - left subclavian artery; 3 - aortic arch; 4 - left pulmonary veins; 5 - left ear; 6 - left coronary artery; 7 - pulmonary artery (cut off); 8 - left ventricle; 9 - apex of the heart; 10 - the descending aorta; 11 - inferior vena cava; 12 - right ventricle; 13 - the right coronary artery; 14 - right ear; 15 - ascending aorta; 16 - superior vena cava; 17 - unnamed artery
Rice. 226. Heart (back view). 1 - aortic arch; 2 - left subclavian artery; 3 - left common carotid artery; 4 - azygos vein; 5 - superior vena cava; 6 - right pulmonary veins; 7 - inferior vena cava; 8 - right atrium; 9 - right coronary artery; 10 - middle vein of the heart; 11 - the descending branch of the right coronary artery; 12 - right ventricle; 13 - apex of the heart; 14 - the diaphragmatic surface of the heart; 15 - left ventricle; 16-17 - total drainage of the heart veins (coronary sinus); 18 - left atrium; 19 - left pulmonary veins; 20 - branches of the pulmonary artery
The right atrium communicates with the right ventricle through the right atrioventricular opening (ostium atrioventriculare dextrum); and the left atrium with the left ventricle - through the left atrioventricular opening (ostium atrioventriculare sinistrum).
The upper part of the right atrium is the right ear of the heart (auricula cordis dextra), which looks like a flattened cone and is located on the anterior surface of the heart, covering the aortic root. In the cavity of the right ear, the muscle fibers of the atrial wall form parallel muscle ridges.
The left heart ear (auricula cordis sinistra) departs from the anterior wall of the left atrium, in the cavity of which there are also muscle ridges. The walls in the left atrium are smoother from the inside than in the right.
The inner shell (Fig. 227), lining the inside of the heart cavity, is called the endocardium (endocardium); it is covered with a layer of endothelium (a derivative of the mesenchyme), extending to the inner lining of the vessels extending from the heart. On the border between the atria and the ventricles, there are thin lamellar outgrowths of the endocardium; here the endocardium, as if folded in half, forms strongly protruding folds, also covered with endothelium on both sides, these are the heart valves (Fig. 228) that close the atrioventricular openings. In the right atrioventricular opening there is a tricuspid valve (valvula tricuspidalis), consisting of three parts - thin fibrous elastic plates, and in the left - a bicuspid valve (valvula bicuspidalis, s. Mytralis), consisting of two of the same plates. These leaflet valves open during atrial systole only towards the ventricles.
Rice. 227. Heart of an adult with ventricles opened in front. 1 - ascending aorta; 2 - arterial ligament (duct overgrown with botallus); 3 - pulmonary artery; 4 - semilunar valves of the pulmonary artery; 5 - left ear of the heart; 6 - front flap of the bivalve valve; 7 - anterior papillary muscle; 8 - back flap of the bivalve valve; 9 - tendon threads; 10 - posterior papillary muscle; 11 - left ventricle of the heart; 12 - the right ventricle of the heart; 13 - back flap of the tricuspid valve; 14 - medial leaf of the tricuspid valve; 15 - right atrium; 16 - anterior cusp of the tricuspid valve, 17 - arterial cone; 18 - right ear
Rice. 228. Heart valves. Opened heart. The direction of blood flow is shown by arrows. 1 - bicuspid valve of the left ventricle; 2 - papillary muscles; 3 - semilunar valves; 4 - tricuspid valve of the right ventricle; 5 - papillary muscles; 6 - aorta; 7 - superior vena cava; 8 - pulmonary artery; 9 - pulmonary veins; 10 - coronary vessels
At the exit site of the aorta from the left ventricle and the pulmonary artery from the right ventricle, the endocardium also forms very thin folds in the form of concave (into the cavity of the ventricle) semicircular pockets, three in each hole. In their shape, these valves are called semilunar (valvulae semilunares). They open only upward towards the vessels during the contraction of the ventricles. During the relaxation (expansion) of the ventricles, they automatically shut down and do not allow the return flow of blood from the vessels to the ventricles; when the ventricles are compressed, they are reopened by the current of the ejected blood. The semilunar valves are devoid of musculature.
From what has been said, it can be seen that in humans, like in other mammals, the heart has four valve systems: two of them, the cusps, separate the ventricles from the atria, and two, semilunar, separate the ventricles from the arterial system. There are no valves at the place where the pulmonary veins enter the left atrium; but the veins approach the heart at an acute angle in such a way that the thin wall of the atrium forms a fold that acts in part as a valve or flap. In addition, there are thickening of the annular muscle fibers of the adjacent part of the atrial wall. This thickening of muscle tissue during atrial contraction compresses the veins and thereby prevents blood from flowing back into the veins so that it only enters the ventricles.
In an organ that does so much work like the heart, support structures naturally develop, to which the muscle fibers of the heart muscle are attached. This soft cardiac "skeleton" includes: tendon rings around its holes, equipped with valves, fibrous triangles located at the root of the aorta and the membranous part of the ventricular septum; they all consist of bundles of collagen fibrils mixed with elastic fibers.
The valves of the heart are composed of dense and elastic connective tissue (duplication of the endocardium - duplication). When the ventricles contract, the cusp valves, under the pressure of blood in the ventricular cavity, expand, like stretched sails, and touch so tightly that they completely close the openings between the atrial cavities and the ventricular cavities. At this time, the tendon threads mentioned above support them and prevent them from turning inside out. Therefore, blood from the ventricles back into the atria cannot get, it is pushed out of the left ventricle into the aorta under the pressure of the contracting ventricles, and from the right ventricle into the pulmonary artery. Thus, all heart valves open only in one direction - in the direction of blood flow.
The size of the cavities of the heart, depending on the degree of filling with blood and the intensity of its work, changes. So, the capacity of the right atrium ranges from 110-185 cm 3. the right ventricle - from 160 to 230 cm 3. the left atrium - from 100 to 130 cm 3 and the left ventricle - from 143 to 212 cm 3.
The heart is covered with a thin serous membrane, forming two sheets, passing one into the other at the place where large vessels leave the heart. The inner, or visceral, leaf of this sac, which directly covers the heart and is tightly welded to it, is called the epicardium (epieardium), the outer, or parietal, leaf is called the pericardium (pericardium). The parietal leaf forms a sac that encloses the heart - this is a heart bag, or a heart shirt. The pericardium from the lateral sides adjoins the leaves of the mediastinal pleura, from below it grows to the tendon center of the diaphragm, and in front is attached by connective tissue fibers to the posterior surface of the sternum. Between both sheets of the cardiac sac around the heart, a slit-like hermetically sealed cavity is formed, always containing a certain amount (about 20 g) of serous fluid. The pericardium isolates the heart from the surrounding organs, and the fluid moisturizes the surface of the heart, reducing friction and making it slide as it contracts. In addition, the strong fibrous tissue of the pericardium limits and prevents excessive stretching of the muscle fibers of the heart; if it were not for the pericardium, which anatomically limits the volume of the heart, it would be in danger of excessive stretching, especially during periods of its most intense and unusual activity.
Incoming and outgoing vessels of the heart. The superior and inferior vena cava enter the right atrium. At the confluence of these veins, a wave of contraction of the heart muscle arises, quickly covering both atria and then passing to the ventricles. In addition to the great vena cava, the coronary sinus of the heart (sinus eoronarius cordis) also flows into the right atrium, through which venous blood flows here from the walls of the heart itself. The sinus opening is closed with a small fold (tebesium flap).
For four years, intramural veins flow into the left atrium. The largest artery in the body, the aorta, leaves the left ventricle. It goes first to the right and up, then, bending back and to the left, it spreads over the left bronchus in the form of an arc. The pulmonary artery leaves the right ventricle; it goes first to the left and up, then turns to the right and divides into two branches, heading to both lungs.
In total, the heart has seven inlet - venous - openings and two outlet - arterial - openings.
Circles of blood circulation(fig. 229). Due to the long and complex evolution of the development of the circulatory organs, a certain system of supplying the body with blood has been established, which is characteristic of humans and all mammals. As a rule, blood moves inside a closed system of tubes, which includes a constantly acting powerful muscular organ - the heart. The heart, as a result of its historically established automatism and regulation by the central nervous system, continuously and rhythmically drives blood throughout the body.
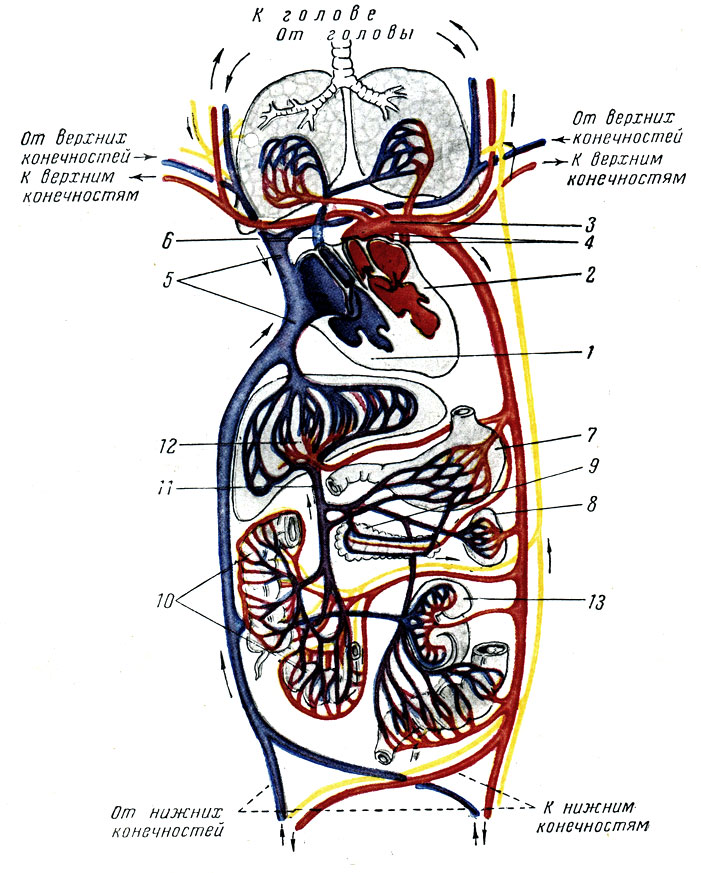
Rice. 229. The scheme of blood circulation and lymph circulation. The vessels through which the arterial blood flows are marked in red; blue - vessels with venous blood; the portal vein system is shown in purple; yellow - lymphatic vessels. 1 - the right half of the heart; 2 - the left half of the heart; 3 - aorta; 4 - pulmonary veins; superior and inferior vena cava; 6 - pulmonary artery; 7 - stomach; 8 - spleen; 9 - pancreas; 10 - intestines; 11 - portal vein; 12 - liver; 13 - kidney
Blood from the left ventricle of the heart through the aorta first enters the large arteries, which gradually branch into smaller ones and then pass into the arterioles and capillaries. Through the thinnest walls of the capillaries, there is a constant exchange of substances between the blood and body tissues. Passing through a dense and numerous network of capillaries, the blood gives oxygen and nutrients to the tissues, and takes carbon dioxide and products of cellular metabolism in return. Changing in its composition, blood later becomes unsuitable for maintaining respiration and nutrition of cells, it turns from arterial to venous. The capillaries begin to gradually merge first into venules, venules into small veins, and the latter into large venous vessels - the superior and inferior vena cava, through which blood returns to the right atrium of the heart, thus describing the so-called large, or corporal, circle of blood circulation.
The venous blood that has entered the right atrium into the right ventricle is sent by the heart through the pulmonary artery to the lungs, where it is freed from carbon dioxide in the smallest network of pulmonary capillaries and saturated with oxygen, and then returns through the pulmonary veins to the left atrium, and from there to the left ventricle of the heart. from where it comes again to supply body tissues. The circulation of blood on the way from the heart through the lungs and back is a small circle of blood circulation. The heart not only performs the work of a motor, but also acts as an apparatus that controls the movement of blood. Switching blood from one circle to another is achieved (in mammals and birds) by the complete separation of the right (venous) half of the heart from the left (arterial) half of it.
These phenomena in the circulatory system have become known to science since the time of Harvey, who discovered (1628) blood circulation, and Malpighi (1661), who established blood circulation in the capillaries.
Blood supply to the heart(see fig. 226). The heart, carrying an extremely important service in the body and doing a great job, itself needs abundant nutrition. It is an organ that is active throughout a person's life and never has a rest period that lasts more than 0.4 seconds. Naturally, this organ must be supplied with a particularly abundant amount of blood. Therefore, its blood supply is arranged in such a way that it completely ensures the inflow and outflow of blood.
The heart muscle receives blood before all other organs through the two coronary (coronary) arteries (a. Eoronaria cordis dextra et sinistra), extending directly from the aorta just above the semilunar valves. In the abundantly developed network of coronary vessels of the heart, even at rest, about 5-10% of all blood ejected into the aorta enters. The right coronary artery along the transverse groove is directed to the right to the posterior half of the heart. It feeds most of the right ventricle, the right atrium, and part of the posterior side of the left heart. Its branch feeds the conducting system of the heart - the Ashof-Tavara node, the bundle of His (see below). The left coronary artery is divided into two branches. One of them goes along the longitudinal groove to the apex of the heart, giving numerous lateral branches, the other goes along the transverse groove to the left and posteriorly to the posterior longitudinal groove. The left coronary artery feeds most of the left heart and the anterior portion of the right ventricle. The coronary arteries disintegrate into a large number of branches, widely aiastomosed among themselves and crumbling into a very dense network of capillaries, penetrating everywhere, in all parts of the organ. The heart has 2 times more (thicker) capillaries than the skeletal muscle.
Venous blood flows from the heart through numerous channels, of which the most significant is the coronary sinus (or a special coronary vein - sinus coronarius cordis), which flows independently directly into the right atrium. All other veins that collect blood from individual parts of the heart muscle also open directly into the heart cavity: into the right atrium, into the right and even into the left ventricle. It turns out that 3/5 of all blood passing through the coronary vessels flows through the coronary sinus, while the rest 2/5 of the blood is collected by other venous trunks.
The heart is also permeated with the richest network of lymphatic vessels. The entire space between the muscle fibers and the blood vessels of the heart is a dense network of lymphatic vessels and crevices. Such an abundance of lymphatic vessels is necessary for the rapid removal of metabolic products, which is very important for the heart as an organ that works continuously.
From the above, it is clear that the heart has its own third circle of blood circulation. Thus, the coronary circle is included in parallel to the entire large circle of blood circulation.
The coronary circulation, in addition to nourishing the heart, also has a protective value for the body, largely mitigating the harmful effects of excessively high blood pressure with a sudden contraction (spasm) of many peripheral vessels of the systemic circulation; in this case, a significant part of the blood is directed along a parallel short and widely branched coronary pathway.
Innervation of the heart(fig. 230). Contractions of the heart are performed automatically due to the properties of the heart muscle. But the regulation of its activity, depending on the needs of the body, is carried out by the central nervous system. IP Pavlov said that "the activity of the heart is controlled by four centrifugal nerves: slowing down, accelerating, weakening and strengthening." These nerves approach the heart as branches from the vagus nerve and from the nodes of the cervical and thoracic regions of the sympathetic trunk. The branches of these nerves form a plexus (plexus cardiacus) on the heart, the fibers of which spread along with the coronary vessels of the heart.
Rice. 230. Conductive system of the heart. The layout of the conducting system in the human heart. 1 - Kis-Flak knot; 2 - Ashof-Tavara node; 3 - bundle of His; 4 - the legs of the bundle of His; 5 - a network of Purkinje fibers; 6 - superior vena cava; 7 - inferior vena cava; 8 - atria; 9 - ventricles
The coordination of the activity of the parts of the heart, atria, ventricles, the sequence of contractions, relaxations are carried out by a special conducting system peculiar only to the heart. The heart muscle has the feature that impulses are conducted to the muscle fibers through special atypical muscle fibers called Purkinje fibers, which form the cardiac conduction system. Purkinje fibers are similar in structure to muscle fibers and directly pass into them. They look like wide ribbons, are poor in myofibrils and are very rich in sarcoplasm. Between the right ear and the superior vena cava, these fibers form a sinus node (Kis-Flak node), which is connected by a bundle of the same fibers to another node (Ashof-Tavara node) located on the border between the right atrium and the ventricle. A large bundle of fibers (His bundle) departs from this node, which descends in the ventricular septum, dividing into two legs, and then crumbles in the walls of the right and left ventricles under the epicardium, ending in the papillary muscles.
The fibers of the nervous system come into close contact with the Purkinje fibers everywhere.
The bundle of His is the only muscular connection between the atrium and the ventricle; through it, the initial stimulus arising in the sinus node is transmitted to the ventricle and ensures the fullness of the cardiac contraction.
1. Functions and development of the cardiovascular system
2. The structure of the heart
3. The structure of the arteries
4. The structure of the veins
5. Microcirculatory bed
6. Lymphatic vessels
1. Cardiovascular system formed by the heart, blood and lymph vessels.
Functions of the cardiovascular system:
· Transport - ensuring the circulation of blood and lymph in the body, transporting them to and from organs. This fundamental function consists of trophic (delivery of nutrients to organs, tissues and cells), respiratory (transport of oxygen and carbon dioxide) and excretory (transport of end products of metabolism to the excretory organs) functions;
· Integrative function - the unification of organs and organ systems into a single organism;
· Regulatory function, along with the nervous, endocrine and immune systems, the cardiovascular system is one of the regulatory systems of the body. It is able to regulate the functions of organs, tissues and cells by delivering mediators, biologically active substances, hormones and others to them, as well as by changing the blood supply;
· The cardiovascular system is involved in immune, inflammatory and other general pathological processes (metastasis of malignant tumors and others).
Development of the cardiovascular system
Vessels develop from the mesenchyme. Distinguish between primary and secondary angiogenesis... Primary angiogenesis, or vasculogenesis, is the process of direct, initial formation of the vascular wall from the mesenchyme. Secondary angiogenesis is the formation of blood vessels by their regrowth from existing vascular structures.
Primary angiogenesis
Blood vessels form in the wall of the yolk sac on
The 3rd week of embryogenesis under the inductive influence of the endoderm that is part of it. First, islets of blood are formed from the mesenchyme. Islet cells differentiate into two directions:
· Hematogenous line gives rise to blood cells;
· The angiogenic lineage gives rise to primary endothelial cells, which connect to each other and form the walls of blood vessels.
In the body of the embryo, blood vessels develop later (in the second half of the third week) from the mesenchyme, the cells of which turn into endothelial cells. At the end of the third week, the primary blood vessels of the yolk sac are connected to the blood vessels of the body of the embryo. After the start of blood circulation through the vessels, their structure becomes more complicated, in addition to the endothelium, membranes are formed in the wall, consisting of muscle and connective tissue elements.
Secondary angiogenesis represents the growth of new vessels from those already formed. It is divided into embryonic and postembryonic. After the endothelium is formed as a result of primary angiogenesis, the further formation of vessels occurs only due to secondary angiogenesis, that is, by regrowth from already existing vessels.
Features of the structure and functioning of different vessels depends on the hemodynamic conditions in a given area of the human body, for example: the level of blood pressure, blood flow velocity, and so on.
The heart develops from two sources: the endocardium is formed from the mesenchyme and at first has the form of two vessels - mesenchymal tubes, which later merge to form the endocardium. The myocardium and mesothelium of the epicardium develop from the myoepicardial plate - part of the visceral sheet of the splanchnotome. The cells of this plate differentiate in two directions: myocardial rudiment and epicardial mesothelium rudiment. The rudiment takes an internal position, its cells turn into cardiomyoblasts capable of division. In the future, they gradually differentiate into three types of cardiomyocytes: contractile, conducting and secretory. The mesothelium of the epicardium develops from the rudiment of the mesothelium (mesothelium). Loose fibrous unformed connective tissue of the epicardial lamina propria is formed from the mesenchyme. Two parts - the mesodermal (myocardium and epicardium) and the mesenchymal (endocardium) join together to form the heart, which consists of three membranes.
2. Heart - it is a kind of pump of rhythmic action. The heart is the central organ of the blood and lymph circulation. In its structure, there are features of both a layered organ (has three membranes) and a parenchymal organ: the stroma and parenchyma can be distinguished in the myocardium.
Heart functions:
· Pumping function - constantly decreasing, maintains a constant level of blood pressure;
Endocrine function - the production of natriuretic factor;
· Information function - the heart encodes information in the form of parameters of blood pressure, blood flow velocity and transmits it to tissues, changing metabolism.
The endocardium consists from four layers: endothelial, subendothelial, muscular-elastic, external connective tissue. Epithelial the layer lies on the basement membrane and is represented by a single-layer squamous epithelium. Subendothelial the layer is formed by loose fibrous loose connective tissue. These two layers are analogous to the inner lining of a blood vessel. Muscular-elastic the layer is formed by smooth myocytes and a network of elastic fibers, an analogue of the middle membrane of blood vessels ... External connective tissue the layer is formed by loose fibrous unformed connective tissue and is analogous to the outer shell of the vessel. It connects the endocardium to the myocardium and continues into its stroma.
Endocardium forms duplicates - heart valves - dense plates of fibrous connective tissue with a small content of cells, covered with endothelium. The atrial side of the valve is smooth, while the ventricular side is uneven, has outgrowths to which tendon filaments are attached. The blood vessels in the endocardium are located only in the outer connective tissue layer, therefore, its nutrition is carried out mainly by the diffusion of substances from the blood, which is located both in the heart cavity and in the vessels of the outer layer.
Myocardium is the most powerful shell of the heart, it is formed by cardiac muscle tissue, the elements of which are cardiomyocyte cells. The set of cardiomyocytes can be considered as myocardial parenchyma. The stroma is represented by interlayers of loose fibrous loose connective tissue, which are normally poorly expressed.
Cardiomyocytes are divided into three types:
· The bulk of the myocardium is made up of working cardiomyocytes, they have a rectangular shape and are connected to each other with the help of special contacts - insertion disks. Due to this, they form a functional synthesia;
· Conducting or atypical cardiomyocytes form the conducting system of the heart, which provides a rhythmic coordinated contraction of its various parts. These cells are genetically and structurally muscular, functionally resemble nerve tissue, as they are capable of forming and rapidly conducting electrical impulses.
There are three types of conducting cardiomyocytes:
· P-cells (pacemaker cells) form a sinoauricular node. They differ from working cardiomyocytes in that they are capable of spontaneous depolarization and the formation of an electrical impulse. The wave of depolarization is transmitted through the nexuses to typical atrial cardiomyocytes, which contract. In addition, excitation is transmitted to intermediate atypical cardiomyocytes of the atrioventricular node. Generation of impulses by P-cells occurs at a frequency of 60-80 per minute;
· Intermediate (transitional) cardiomyocytes of the atrioventricular node transmit excitation to working cardiomyocytes, as well as to the third type of atypical cardiomyocytes - Purkinje fiber cells. Transient cardiomyocytes are also capable of independently generating electrical impulses, but their frequency is lower than the frequency of impulses generated by pacemaker cells, and leaves 30-40 per minute;
· Fiber cells - the third type of atypical cardiomyocytes, of which the His bundle and Purkinje fibers are built. The main function of fiber cells is the transmission of excitation from intermediate atypical cardiomyocytes to working ventricular cardiomyocytes. In addition, these cells are capable of independently generating electrical impulses with a frequency of 20 or less per minute;
· Secretory cardiomyocytes are located in the atria, the main function of these cells is the synthesis of natriuretic hormone. It is released into the blood when a large amount of blood enters the atrium, that is, when there is a threat of increased blood pressure. Released into the bloodstream, this hormone acts on the kidney tubules, preventing the reverse reabsorption of sodium into the blood from the primary urine. At the same time, water is released from the body in the kidneys along with sodium, which leads to a decrease in the volume of circulating blood and a drop in blood pressure.
Epicard- the outer shell of the heart, it is the visceral layer of the pericardium - the heart bag. The epicardium consists of two sheets: the inner layer, represented by loose fibrous loose connective tissue, and the outer layer, a single-layer squamous epithelium (mesothelium).
Blood supply to the heart carried out by the coronary arteries originating from the aortic arch. Coronary arteries have a highly developed elastic frame with pronounced external and internal elastic membranes. The coronary arteries branch strongly to capillaries in all membranes, as well as in the papillary muscles and tendon cords of the valves. Vessels are also contained at the base of the heart valves. From the capillaries, blood is collected in the coronary veins, which pour blood either into the right atrium or into the venous sinus. An even more intensive blood supply has a conductive system, where the density of capillaries per unit area is higher than in the myocardium.
Features of lymphatic drainage of the heart is that in the epicardium the lymphatic vessels accompany the blood vessels, while in the endocardium and myocardium they form their own abundant networks. Lymph from the heart flows into the lymph nodes in the area of the aortic arch and the lower trachea.
The heart receives both sympathetic and parasympathetic innervation.
Stimulation of the sympathetic part of the autonomic nervous system causes an increase in strength, heart rate and the rate of conduction of excitation through the heart muscle, as well as expansion of the coronary vessels and an increase in the blood supply to the heart. Stimulation of the parasympathetic nervous system causes effects opposite to those of the sympathetic nervous system: a decrease in the frequency and strength of heart contractions, myocardial excitability, narrowing of the coronary vessels with a decrease in the blood supply to the heart.
3. Blood vessels are organs of the layered type. They consist of three membranes: inner, middle (muscular) and outer (adventitious). Blood vessels are divided into:
· Arteries that carry blood from the heart;
• veins through which blood moves to the heart;
· Vessels of the microvasculature.
The structure of blood vessels depends on hemodynamic conditions. Hemodynamic conditions- these are the conditions for the movement of blood through the vessels. They are determined by the following factors: blood pressure, blood flow velocity, blood viscosity, exposure gravitational field Earth, the location of the vessel in the body. Hemodynamic conditions determine such morphological signs of blood vessels as:
· Wall thickness (in the arteries it is more, and in the capillaries - less, which facilitates the diffusion of substances);
· The degree of development of the muscular membrane and the direction of smooth myocytes in it;
· The ratio in the middle shell of the muscle and elastic components;
· Presence or absence of inner and outer elastic membranes;
· The depth of the vessels;
· Presence or absence of valves;
· The ratio between the thickness of the vessel wall and the diameter of its lumen;
· The presence or absence of smooth muscle tissue in the inner and outer shells.
By the diameter of the artery are divided into arteries of small, medium and large caliber. According to the quantitative ratio in the middle shell of the muscular and elastic components, they are subdivided into elastic, muscular and mixed arteries.
Elastic type arteries
These vessels include the aorta and pulmonary arteries; they perform the transport function and the function of maintaining pressure in the arterial system during diastole. In this type of vessels, the elastic frame is highly developed, which allows the vessels to stretch strongly, while maintaining the integrity of the vessel.
Elastic type arteries are built according to the general principle of the structure of blood vessels and consist of an inner, middle and outer shell. Inner shell rather thick and formed by three layers: endothelial, podendothelial and elastic fiber layer. In the endothelial layer, the cells are large, polygonal; they lie on the basement membrane. The podendothelial layer is formed by loose fibrous loose connective tissue, which contains many collagen and elastic fibers. The inner elastic membrane is missing. Instead, on the border with the middle shell is a plexus of elastic fibers, consisting of an inner circular and outer longitudinal layers. The outer layer passes into the plexus of elastic fibers of the middle shell.
Middle shell consists mainly of elastic elements. In an adult, they form 50-70 fenestrated membranes, which lie at a distance of 6-18 microns from each other and each have a thickness of 2.5 microns. Loose fibrous unformed connective tissue with fibroblasts, collagen, elastic and reticular fibers, smooth myocytes is located between the membranes. In the outer layers of the middle shell are the vessels of the vessels that feed the vascular wall.
Outer adventitia relatively thin, consists of loose fibrous loose connective tissue, contains thick elastic fibers and bundles of collagen fibers running longitudinally or obliquely, as well as vascular vessels and vascular nerves formed by myelin and myelin-free nerve fibers.
Arteries of mixed (muscular-elastic) type
An example of a mixed type artery is the axillary and carotid arteries. Since the pulse wave gradually decreases in these arteries, along with the elastic component, they have a well-developed muscle component to maintain this wave. The wall thickness in these arteries increases significantly in comparison with the diameter of the lumen.
Inner shell represented by endothelial, subendothelial layers and an internal elastic membrane. In the middle shell both muscular and elastic components are well developed. Elastic elements are represented by individual fibers that form a network, fenestrated membranes and layers of smooth myocytes lying between them, running in a spiral. Outer sheath formed by loose fibrous loose connective tissue, in which bundles of smooth myocytes are found, and an external elastic membrane lying immediately behind the middle membrane. The outer elastic membrane is somewhat less pronounced than the inner one.
Muscular arteries
These arteries include arteries of small and medium caliber lying near organs and intraorgan. In these vessels, the strength of the pulse wave is significantly reduced, and it becomes necessary to create additional conditions for the advancement of blood, therefore, the muscle component predominates in the middle shell. The diameter of these arteries can decrease due to contraction and increase due to relaxation of smooth myocytes. The wall thickness of these arteries significantly exceeds the diameter of the lumen. Such vessels create resistance to the driving blood, which is why they are often called resistive.
Inner shell has a small thickness and consists of endothelial, podendothelial layers and an internal elastic membrane. Their structure is generally the same as in mixed type arteries, and the inner elastic membrane consists of one layer of elastic cells. The middle shell consists of smooth myocytes arranged in a gentle spiral, and a loose network of elastic fibers, also spiraling. The spiral arrangement of myocytes contributes to a greater decrease in the lumen of the vessel. The elastic fibers merge with the outer and inner elastic membranes to form a single frame. Outer sheath formed by an external elastic membrane and a layer of loose fibrous loose connective tissue. It contains blood vessels of blood vessels, sympathetic and parasympathetic nerve plexuses.
4. The structure of the veins, as well as arteries, depends on hemodynamic conditions. In the veins, these conditions depend on whether they are located in the upper or lower body, since the structure of the veins of these two zones is different. There are veins of the muscular and non-muscular types. To the veins of the muscleless type include the veins of the placenta, bones, pia mater, retina, nail bed, trabeculae of the spleen, central veins of the liver. The absence of a muscular membrane in them is explained by the fact that the blood here moves under the influence of gravity, and its movement is not regulated by muscle elements. These veins are built from the inner membrane with the endothelium and podendothelial layer and the outer membrane of loose fibrous loose connective tissue. The inner and outer elastic membranes, as well as the middle shell, are absent.
Veins of the muscle type are subdivided into:
· Veins with poor development of muscle elements, these include small, medium and large veins of the upper body. Veins of small and medium caliber with poor muscular development are often located intraorgan. The podendothelial layer in small and medium-sized veins is relatively poorly developed. Their muscular membrane contains a small number of smooth myocytes, which can form separate clusters that are distant from each other. The sections of the vein between such clusters are able to expand sharply, performing a depositing function. The middle shell is represented by a small amount of muscle elements, the outer shell is formed by loose fibrous loose connective tissue;
Veins with medium development of muscle elements, an example of this type of vein is the brachial vein. The inner membrane consists of the endothelial and subendothelial layers and forms duplicate valves with a large number of elastic fibers and smooth myocytes located longitudinally. The inner elastic membrane is absent; it is replaced by a network of elastic fibers. The middle shell is formed by spirally lying smooth myocytes and elastic fibers. The outer membrane is 2-3 times thicker than that of the artery, and it consists of longitudinally lying elastic fibers, individual smooth myocytes and other components of loose fibrous unformed connective tissue;
Veins with a strong development of muscle elements, an example of this type of veins are the veins of the lower body - the inferior vena cava, the femoral vein. These veins are characterized by the development of muscle elements in all three membranes.
5. Microcirculatory bed includes the following components: arterioles, precapillaries, capillaries, postcapillaries, venules, arterio-venular anastomoses.
The functions of the microvasculature are as follows:
Trophic and respiratory functions, since the exchange surface of capillaries and venules is 1000 m2, or 1.5 m2 per 100 g of tissue;
· Depositing function, since a significant part of the blood is deposited in the vessels of the microvasculature at rest, which is included in the bloodstream during physical work;
· Drainage function, since the microvasculature collects blood from the bringing arteries and distributes it throughout the organ;
· Regulation of blood flow in the organ, this function is performed by arterioles due to the presence of sphincters in them;
· Transport function, that is, blood transport.
Three links are distinguished in the microvasculature: arterial (arterioles precapillaries), capillary and venous (postcapillaries, collecting and muscle venules).
Arterioles have a diameter of 50-100 microns. In their structure, three membranes are preserved, but they are less pronounced than in the arteries. In the area where the capillary arteriole leaves, there is a smooth muscle sphincter that regulates blood flow. This area is called the precapillary.
Capillaries- these are the smallest vessels, they vary in size on the:
· Narrow type 4-7 microns;
· Normal or somatic type 7-11 microns;
· Sinusoidal type 20-30 microns;
· Lacunar type 50-70 microns.
A layered principle is traced in their structure. The inner layer is formed by the endothelium. The endothelial layer of the capillary is an analogue of the inner shell. It lies on the basement membrane, which first splits into two sheets and then joins. As a result, a cavity is formed in which pericyte cells lie. On these cells, these cells end with autonomic nerve endings, under the regulatory action of which the cells can accumulate water, increase in size and close the lumen of the capillary. When water is removed from the cells, they decrease in size, and the lumen of the capillaries opens. Functions of pericytes:
· Change in the lumen of the capillaries;
· Source of smooth muscle cells;
· Control of proliferation of endothelial cells during capillary regeneration;
· Synthesis of components of the basement membrane;
· Phagocytic function.
Basement membrane with pericytes- analogue of the middle shell. Outside of it is a thin layer of the basic substance with adventitia cells, which play the role of a cambium for loose fibrous unformed connective tissue.
Organ specificity is characteristic of capillaries, and therefore three types of capillaries:
Capillaries of the somatic type or continuous, they are located in the skin, muscles, brain, spinal cord... They are characterized by a continuous endothelium and a continuous basement membrane;
Capillaries of fenestrated or visceral type (localization - internal organs and endocrine glands). They are characterized by the presence of constrictions in the endothelium - fenestra and a continuous basement membrane;
Intermittent or sinusoidal capillaries (red Bone marrow, spleen, liver). In the endothelium of these capillaries there are true openings, they are also in the basement membrane, which may be absent altogether. Sometimes capillaries include lacunas - large vessels with a wall structure like in a capillary (cavernous bodies of the penis).
Venules are divided into postcapillary, collective and muscular. Postcapillary venules are formed as a result of the fusion of several capillaries, have the same structure as a capillary, but a larger diameter (12-30 microns) and a large number of pericytes. In the collecting venules (diameter 30-50 microns), which are formed when several postcapillary venules merge, there are already two pronounced membranes: the inner one (endothelial and subendothelial layers) and the outer one - loose fibrous unformed connective tissue. Smooth myocytes appear only in large venules reaching a diameter of 50 μm. These venules are called muscle venules and are up to 100 microns in diameter. Smooth myocytes in them, however, do not have a strict orientation and form a single layer.
Arterio-venular anastomoses or shunts- this is a type of vessels in the microcirculatory bed, through which blood from arterioles enters the venules, bypassing the capillaries. This is necessary, for example, in the skin for thermoregulation. All arterio-venular anastomoses are divided into two types:
• true - simple and complex;
· Atypical anastomoses or shunts.
In simple anastomoses there are no contractile elements, and the blood flow in them is regulated by the sphincter located in the arterioles at the site of the anastomosis. In complex anastomoses there are elements in the wall that regulate their lumen and the intensity of blood flow through the anastomosis. Complex anastomoses are divided into glomus-type anastomoses and trailing artery-type anastomoses. In anastomoses of the type of guard arteries in the inner membrane there are accumulations of longitudinally smooth myocytes. Their contraction leads to protrusion of the wall in the form of a pillow into the lumen of the anastomosis and its closure. In anastomoses such as the glomerulus (glomerulus), there is an accumulation of epithelioid E-cells (in the form of an epithelium) in the wall, capable of sucking in water, increasing in size and closing the lumen of the anastomosis. With the release of water, the cells decrease in size, and the lumen opens. There are no contractile elements in the half-shunts in the wall, the width of their lumen is not regulated. Venous blood from venules can be thrown into them, therefore mixed blood flows in half shunts, in contrast to shunts. Anastomoses perform the function of blood redistribution, blood pressure regulation.
6. Lymphatic system conducts lymph from tissues to the venous bed. It consists of lymphocapillaries and lymphatic vessels. Lymphocapillaries start blindly in tissues. Their wall often consists only of the endothelium. The basement membrane is usually absent or poorly expressed. In order to prevent the capillary from collapsing, there are sling or anchor filaments, which are attached to endotheliocytes at one end, and are woven into loose fibrous connective tissue at the other. The diameter of the lymphocapillaries is 20-30 microns. They perform a drainage function: they suck in tissue fluid from the connective tissue.
Lymphatic vessels divided into intraorganic and extraorganic, as well as the main (chest and right lymphatic ducts). By diameter, they are divided into small, medium and large lymphatic vessels. In vessels of small diameter, there is no muscular sheath, and the wall consists of an inner and an outer shell. The inner shell consists of the endothelial and subendothelial layers. The subendothelial layer is gradual, without sharp boundaries. It passes into a loose fibrous unformed connective tissue of the outer shell. Vessels of medium and large caliber have a muscular membrane and are similar in structure to veins. The large lymphatic vessels have elastic membranes. The inner shell forms the valves. In the course of the lymphatic vessels, there are lymph nodes, the passages through which, the lymph is cleansed and enriched with lymphocytes.
Anatomy and physiology of the cardiovascular systemThe cardiovascular system includes the heart as a hemodynamic apparatus, arteries through which blood is delivered to the capillaries, which ensure the exchange of substances between blood and tissues, and veins, which deliver blood back to the heart. Due to the innervation of autonomic nerve fibers, a connection is made between the circulatory system and the central nervous system (CNS).
The heart is a four-chambered organ, its left half (arterial) consists of the left atrium and left ventricle, which do not communicate with its right half (venous), consisting of the right atrium and right ventricle. The left half distills blood from the veins of the pulmonary circulation into the artery of the large circle, and the right half distills blood from the veins of the large circle into the artery of the pulmonary circulation. In a healthy adult, the heart is located asymmetrically; about two thirds are to the left of the midline and are represented by the left ventricle, most of the right ventricle and left atrium, and the left ear (Fig. 54). One third is located to the right and represents the right atrium, a small portion of the right ventricle, and a small portion of the left atrium.
The heart lies in front of the spine and is projected at the level of the IV-VIII thoracic vertebrae. The right half of the heart is facing forward, and the left half is facing back. The anterior surface of the heart is formed by the anterior wall of the right ventricle. On the top right, the right atrium with its ear is involved in its formation, and on the left is a part of the left ventricle and a small part of the left ear. The posterior surface is formed by the left atrium and minor parts of the left ventricle and right atrium.
The heart has a sternocostal, diaphragmatic, pulmonary surface, base, right edge and apex. The latter is free; large blood trunks begin from the base. Four pulmonary veins flow into the left atrium, without a valve apparatus. Both vena cava flows into the right atrium from behind. The superior vena cava has no valves. The inferior vena cava has an Eustachian flap, which does not completely separate the lumen of the vein from the lumen of the atrium. In the cavity of the left ventricle, the left atrioventricular orifice and the aortic mouth are located. Similarly, in the right ventricle, the right atrioventricular orifice and the mouth of the pulmonary artery are located.
Each ventricle consists of two sections - the inflow and outflow tract. The path of blood flow goes from the atrioventricular opening to the apex of the ventricle (right or left); the pathway of blood outflow is located from the apex of the ventricle to the orifice of the aorta or pulmonary artery. The ratio of the length of the inflow path to the length of the outflow path is 2: 3 (channel index). If the cavity of the right ventricle is able to receive a large amount of blood and increase 2-3 times, then the left ventricular myocardium can sharply increase intraventricular pressure.
The cavities of the heart are formed from the myocardium. The atrial myocardium is thinner than the ventricular myocardium and consists of 2 layers of muscle fibers. The ventricular myocardium is more powerful and consists of 3 layers of muscle fibers. Each myocardial cell (cardiomyocyte) is limited by a double membrane (sarcolema) and contains all the elements: the nucleus, myofimbrils and organelles.
The inner shell (endocardium) lines the heart cavity from the inside and forms its valve apparatus. The outer shell (epicardium) covers the outside of the myocardium.
Thanks to the valve apparatus, the blood always flows in one direction during the contraction of the heart muscles, and in diastole it does not return from the large vessels in the ventricular cavity. The left atrium and the left ventricle are separated by a bicuspid (mitral) valve, which has two cusps: a large right and a smaller left. There are three cusps in the right atrioventricular opening.
Large vessels extending from the ventricular cavity have semilunar valves, consisting of three cusps that open and close depending on the blood pressure in the cavities of the ventricle and the corresponding vessel.
Nervous regulation of the heart is carried out with the help of central and local mechanisms. The central ones include the innervation of the vagus and sympathetic nerves. Functionally, the vagus and sympathetic nerves act in exactly the opposite way.
Vagus influence reduces the tone of the heart muscle and the automatism of the sinus node, to a lesser extent the atrioventricular junction, as a result of which the heart contractions are reduced. Slows down the conduction of excitation from the atria to the ventricles.
The sympathetic influence speeds up and intensifies the heart contractions. Also humoral mechanisms influence cardiac activity. Neurohormones (adrenaline, norepinephrine, acetylcholine, etc.) are products of the activity of the autonomic nervous system (neurotransmitters).
The conducting system of the heart is a neuromuscular organization capable of conducting excitation (Fig. 55). It consists of a sinus node, or Kiss-Fleck node, located at the confluence of the superior vena cava under the epicardium; atrioventricular node, or Ashof-Tavar node, located in the lower part of the wall of the right atrium, near the base of the medial leaflet of the tricuspid valve and partially in the lower part of the interatrial and upper part of the interventricular septum. From it down goes the trunk of the bundle of His, located in the upper part of the interventricular septum. At the level of its membrane part, it is divided into two branches: right and left, which later disintegrate into small branches - Purkinje fibers, which join the ventricular muscle. The left bundle branch is divided into anterior and posterior. The anterior branch penetrates the anterior part of the interventricular septum, the anterior and anterolateral walls of the left ventricle. The posterior branch passes into the posterior part of the interventricular septum, the posterior-lateral and posterior walls of the left ventricle.
The blood supply to the heart is carried out by a network of coronary vessels and mostly falls on the left coronary artery, one quarter - on the right, both of them depart from the very beginning of the aorta, located under the epicardium.
The left coronary artery is divided into two branches:
The anterior descending artery, which supplies blood to the anterior wall of the left ventricle and two-thirds of the interventricular septum;
The circumflex artery, which supplies blood to part of the postero-lateral surface of the heart.
The right coronary artery supplies blood to the right ventricle and the posterior surface of the left ventricle.
The sinoatrial node is supplied with blood through the right coronary artery in 55% of cases and through the circumflex coronary artery in 45%. The myocardium is characterized by automatism, conduction, excitability, contractility. These properties determine the work of the heart as a circulatory organ.
Automatism is the ability of the heart muscle itself to generate rhythmic impulses for its contraction. Normally, an excitation pulse originates in the sinus node. Excitability - the ability of the heart muscle to respond by contraction to the impulse passing through it. It is replaced by periods of non-excitability (refractory phase), which ensures a sequence of contraction of the atria and ventricles.
Conductivity - the ability of the heart muscle to conduct an impulse from the sinus node (normal) to the working muscles of the heart. Due to the fact that there are slow conduction of the impulse (in the atrioventricular node), the contraction of the ventricles occurs after the end of the atrial contraction.
The contraction of the heart muscle occurs sequentially: first, the atria (atrial systole) contract, then the ventricles (ventricular systole), after the contraction of each section, it relaxes (diastole).
The volume of blood flowing into the aorta with each contraction of the heart is called systolic, or stroke. The minute volume is the product of the stroke volume and the number of heartbeats per minute. Under physiological conditions, the systolic volume of the right and left ventricles is the same.
Blood circulation - contraction of the heart as a hemodynamic apparatus overcomes resistance in the vascular network (especially in arterioles and capillaries), creates high blood pressure in the aorta, which decreases in arterioles, becomes less in capillaries and even less in veins.
The main factor in the movement of blood is the difference in blood pressure on the way from the aorta to the vena cava; the suction action of the chest and the contraction of skeletal muscles also contribute to the advancement of blood.
Schematically, the main stages of blood advance are:
Atrial contraction;
Contraction of the ventricles;
The advancement of blood through the aorta to large arteries (elastic-type arteries);
The advancement of blood through the arteries (arteries of the muscle type);
Capillary advancement;
Advancement through the veins (which have valves that prevent the retrograde movement of blood);
Atrial inflow.
The height of blood pressure is determined by the force of contraction of the heart and the degree of tonic contraction of the muscles of small arteries (arterioles).
The maximum, or systolic, pressure is reached during ventricular systole; minimum, or diastolic, - by the end of diastole. The difference between systolic and diastolic pressure is called pulse pressure.
Normally, in an adult, the height of blood pressure when measured on the brachial artery is: systolic 120 mm Hg. Art. (with fluctuations from 110 to 130 mm Hg), diastolic 70 mm (with fluctuations from 60 to 80 mm Hg), pulse pressure about 50 mm Hg. Art. The height of the capillary pressure is 16–25 mm Hg. Art. The height of the venous pressure is 4.5 to 9 mm Hg. Art. (or from 60 to 120 mm H2O).
It is better to read this article for those who have at least some idea of the heart, it is written quite hard. I would not recommend it to students. And the circulatory circles are not described in detail. Well, 4+ ...
Heart(cor) is a hollow four-chambered muscular organ that pumps oxygen-enriched blood into the artery and receives venous blood.
The heart consists of two atria that receive blood from the veins and push it into the ventricles (right and left). The right ventricle supplies blood to pulmonary arteries through the pulmonary trunk, and the left one into the aorta. The left half of the heart contains arterial blood, and the right half of the heart contains venous blood, the right and left halves of the heart are not normally communicated.
The heart is distinguished: three surfaces - pulmonary (facies pulmonalis), sternocostal (facies sternocostalis) and diaphragmatic (facies diaphragmatica); the top (apex cordis) and the base (basis cordis). The border between the atria and the ventricles is the coronary sulcus (sulcus coronarius).
Right atrium(atrium dextrum) is separated from the left by the atrial septum (septum interatriale) and has an additional cavity - the right ear (auricula dextra). There is a depression in the septum - an oval fossa surrounded by the edge of the same name, formed after the oval opening is overgrown.
The right atrium has openings of the superior vena cava (ostium venae cavae superioris) and the inferior vena cava (ostium venae cavae inferioris), delimited by the intervenous tubercle (tuberculum intervenosum) and the opening of the coronary sinus (ostium sinus coronarii). On the inner wall of the right ear there are comb muscles (mm pectinati), ending with a border ridge separating the venous sinus from the cavity of the right atrium.
The right atrium communicates with the ventricle through the right atrioventricular opening (ostium atrioventriculare dextrum).
Right ventricle(ventriculus dexter) is separated from the left interventricular septum (septum interventriculare), in which the muscular and membranous parts are distinguished; has an opening of the pulmonary trunk in front (ostium trunci pulmonalis) and behind - the right atrioventricular opening (ostium atrioventriculare dextrum). The latter is covered with a tricuspid valve (valva tricuspidalis), which has anterior, posterior and septal valves. The leaflets are held in place by tendinous chords, due to which the leaflets are not everted into the atrium.
On the inner surface of the ventricle there are fleshy trabeculae (trabeculae carneae) and papillary muscles (mm. Papillares), from which tendon chords begin. The opening of the pulmonary trunk is covered with a valve of the same name, consisting of three semilunar valves: front, right and left (valvulae semilunares anterior, dextra et sinistra).
Left atrium(atrium sinistrum) has a cone-shaped extension facing anteriorly - the left ear (auricular sinistra) - and five openings: four openings of the pulmonary veins (ostia venarum pulmonalium) and the left atrioventricular opening (ostium atrioventriculare sinistrum).
Left ventricle(ventriculus sinister) has a left atrioventricular opening behind, covered by a mitral valve (valva mitralis), consisting of anterior and posterior cusps, and aortic openings, covered by a valve of the same name, consisting of three semilunar valves: posterior, right and left (valvulae semilunares posterior , dextra et sinistra). There are sinuses between the flaps and the aortic wall. On the inner surface of the ventricle there are fleshy trabeculae (trabeculae carneae), anterior and posterior papillary muscles (mm.papillares anterior et posterior).
2. STRUCTURE OF THE HEART WALL. HEART CONDUCTIVE SYSTEM. STRUCTURE OF THE PERICARDIUM
Wall of the heart consists of a thin inner layer - the endocardium (endocardium), the middle developed layer - the myocardium (myocardium) and the outer layer - the epicardium (epicardium).
The endocardium lines the entire inner surface of the heart with all its formations.
The myocardium is formed by the cardiac striated muscle tissue and consists of cardiac cardiomyocytes, which provides a complete and rhythmic contraction of all chambers of the heart. The muscle fibers of the atria and ventricles start from the right and left (anuli fibrosi dexter et sinister) fibrous rings, which are part of the soft skeleton of the heart. The annulus fibrosus surround the corresponding atrioventricular openings, providing support for their valves.
The myocardium consists of three layers. The outer oblique layer at the apex of the heart passes into the curl of the heart (vortex cordis) and continues into the deep layer. The middle layer is formed by circular fibers. The epicardium is built on the principle of the serous membranes and is the visceral layer of the serous pericardium. The epicardium covers the outer surface of the heart from all sides and the initial sections of the vessels departing from it, passing along them into the parietal plate of the serous pericardium.
The normal contractile function of the heart is provided by conducting system, the centers of which are:
1) sinus-atrial node (nodus sinuatrialis), or Kis-Fleck's node;
2) the atrioventricular node (nodus atrioventricularis), or the Fschoff-Tavara node, passing downward into the atrioventricular bundle (fasciculus atrioventricularis), or the bundle of His, which is divided into the right and left legs (cr dextrum et sinistrum).
Pericardium (pericardium) is a fibro-serous sac in which the heart is located. The pericardium is formed by two layers: the outer (fibrous pericardium) and the inner (serous pericardium). The fibrous pericardium passes into the adventitia of the large vessels of the heart, and the serous one has two plates - parietal and visceral, which pass into each other in the region of the base of the heart. Between the plates there is a pericardial cavity (cavitas pericardialis), it contains a small amount of serous fluid. In the pericardium, three sections are distinguished: the anterior, or sternocostal, right and left mediastinal sections, the lower, or diaphragmatic, section.
The blood supply to the pericardium is carried out in the branches of the superior phrenic arteries, branches of the thoracic aorta, branches of the pericardio-diaphragmatic artery.
Venous outflow is carried out in the azygos and semi-unpaired veins.
Lymphatic drainage is carried out into the anterior and posterior mediastinal, pericardial and pre-pericardial lymph nodes.
Innervation: branches of the right and left sympathetic trunks, branches of the phrenic and vagus nerves.
3. BLOOD SUPPLY AND HEART INERVATION
The arteries of the heart originate from the aortic bulb (bulbus aortae).
The right coronary artery (a coronaria dextra) has a large branch - the posterior interventricular branch (ramus interventricularis posterior).
The left coronary artery (a.coronaria sinistra) is divided into the envelope (r. Circumflexus) n anterior interventricular branches (r. Interventricularis anterior). These arteries combine to form transverse and longitudinal arterial rings.
Small (v. Cordis parva), middle (v. Cordis media) and large veins of the heart (v. Cordis magna), oblique (v. Oblique atrii sinistri) and posterior veins of the left ventricle (v. Posterior ventriculi sinistri) form the coronary sinus ( sinus coronarius). In addition to these veins, there are the smallest (vv. Cordis minimae) and anterior veins of the heart (vv. Cordis anteriores).
Lymphatic drainage is carried out into the anterior mediastinal and one of the lower tracheobronchial lymph nodes.
Innervation:
1) cardiac nerves originating from the cervical and upper thoracic nodes of the right and left lymphatic trunks;
2) superficial extraorganic cardiac plexus;
3) deep extraorganic cardiac plexus;
4) intraorgan cardiac plexus (formed by the branches of extraorgan cardiac plexuses).
4. PULMONARY TRUNK AND ITS BRANCHES. STRUCTURE OF THE AORTA AND ITS BRANCHES
Pulmonary trunk(truncus pulmonalis) is divided into right and left pulmonary arteries. The place of division is called the bifurcation of the pulmonary trunk (bifurcatio trunci pulmonalis).
Right pulmonary artery(a. pulmonalis dextra) enters the gate of the lung and divides. In the upper lobe, the descending and ascending posterior branches (rr. Posteriores descendens et ascendens), the apical branch (r. Apicalis), the descending and ascending front branches (rr. Anteriores descendens et ascendens) are distinguished. In the middle lobe, medial and lateral branches are distinguished (rr.lobi medii medialis et lateralis). In the lower lobe - the upper branch of the lower lobe (r. Superior lobi inferioris) and the basal part (pars basalis), which is divided into four branches: anterior and posterior, lateral and medial.
Left pulmonary artery(a. pulmonalis sinistra), entering the gate of the left lung, is divided into two parts. The ascending and descending front (rr. Anteriores ascendens et descendens), reed (r. Lingularis), back (r. Posterior) and apical branches (r. Apicalis) go to the upper lobe. The upper branch of the lower lobe goes to the lower lobe of the left lung, the basal part is divided into four branches: anterior and posterior, lateral and medial (as in the right lung).
Pulmonary veins originate from the capillaries of the lung.
The right lower pulmonary vein (v. Pulmonalis dextra inferior) collects blood from five segments of the lower lobe of the right lung. This vein forms when the superior vein of the inferior lobe and the common basal vein merge.
The right upper pulmonary vein (v. Pulmonalis dextra superior) collects blood from the upper and middle lobes of the right lung.
The left lower pulmonary vein (v. Pulmonalis sinistra inferior) collects blood from the lower lobe of the left lung.
The left upper pulmonary vein (v. Pulmonalis sinistra superior) collects blood from the upper lobe of the left lung.
The right and left pulmonary veins flow into the left atrium.
Aorta(aorta) has three sections: the ascending part, the arch and the descending part.
Ascending part of the aorta(pars ascendens aortae) has an extension in the initial section - the aortic bulb (bulbus aortae), and at the location of the valve - three sinuses.
Aortic arch(arcus aortae) originates at the level of the articulation of the II right costal cartilage with the sternum; has a slight narrowing, or isthmus of the aorta (isthmus aortae).
Descending part of the aorta(pars descendens aortae) begins at level IV of the thoracic vertebra and continues to IV lumbar vertebra where it divides into the right and left common iliac arteries. In the descending part, the chest (pars thoracica aortae) and abdominal parts (pars abdominalis aortae) are isolated.
5. SHOULDER SHAFT. EXTERNAL CAROTID ARTERY
Brachiocephalic trunk(truncus brachiocephalicus) is located in front of the trachea and behind the right brachiocephalic vein, departing from the aortic arch at level II of the right costal cartilage; at the level of the right sternoclavicular joint, it is divided into the right common carotid and right subclavian arteries, which are its terminal branches. The left common carotid artery (a. Carotis communis sinistra) departs from the aortic arch itself.
External carotid artery(a. carotis externa) is one of the two branches of the common carotid artery, which gives off many branches.
Anterior branches of the external carotid artery .
Superior thyroid artery(a. thyroidea superior) at the upper pole of the thyroid lobe is divided into anterior and posterior branches. This artery has lateral branches:
1) subhyoid branch (r. Infrahyoideus);
2) sternocleidomastoid branch (r. Sternocleidomastoidea);
3) the superior laryngeal artery (a. Laryngea superior);
4) cricothyroid branch (r. Cricothyroideus).
(Lingual artery(a. lingualis) departs at the level of the large horn of the hyoid bone, gives off dorsal branches, and its final branch is the deep artery of the tongue (a. profunda linguae); before entering the language, it gives two more branches: the sublingual artery (a. sublingualis) and the suprahyoid branch (rü suprahyoideus).
Facial artery(ayu facialis) originates just above the lingual artery. The face gives the following branches:
1) the upper labial artery (a. Labialis inferior);
2) lower labial artery (a. Labialis superior);
3) angular artery (a. Angularis).
On the neck, the facial artery gives the following branches:
1) amygdala branch (r. Tonsillaris);
2) chin artery (a. Submentalis);
3) the ascending palatine artery (a. Palatine ascendens).
((bi) Posterior branches of the external carotid artery .
The posterior ear artery (a.auricularis posterior) gives the following branches:
1) the occipital branch (r. Occipitalis);
2) the ear branch (r. Auricularis);
3) the styloid artery (a. Stylomastoidea), giving the posterior tympanic artery (a. Tympanica posterior).
The occipital artery (a.occipitalis) gives the following branches:
1) auricular branch (r. Auricularis);
2) descending branch (r. Descendens);
3) sternocleidomastoid branches (rr.sternocleidomastoidea);
4) mastoid branch (r. Mastoideus).
The ascending pharyngeal artery (a.pharyngea ascendens) gives the following branches:
1) pharyngeal branches (rr. Pharyngealis);
2) the lower tympanic artery (a.tympanica inferior);
3) posterior meningeal artery (a. Meningea posterior).
Terminal branches of the external carotid artery.
Maxillary artery(a. maxillaries), in which there are three sections - jaw, pterygoid, pterygo-palatine, from which their branches branch off.
Branches of the jaw:
1) anterior tympanic artery (a.tympanica anterior);
2) deep ear artery (a. Auricularis profunda);
3) the middle meningeal artery (a. Meningea media), giving the superior tympanic artery (a. Tympanica superior), frontal and parietal branches (rr. Frontalis et parietalis);
4) lower alveolar artery (a.alveolaris inferior).
Pterygoid branches:
1) pterygoid branches (rr. Pterigoidei);
2) the chewing artery (a. Masseterica);
3) buccal artery (a. Buccalis);
4) anterior and posterior temporal arteries (rr. Temporales anterioris et posterioris);
5) the posterior superior alveolar artery (a.alveolaris superior posterior).
Branches of the pterygo-palatine department:
1) the descending palatine artery (a. Palatine descendens);
2) the wedge-palatine artery (a. Sphenopalatina), giving the posterior septal branches (rr. Septales posteriores) and lateral posterior nasal arteries (aa. Nasales posteriores laterales);
3) infraorbital artery (a. Infraorbitalis), giving the anterior superior alveolar arteries (aa. Alveolares superiores anteriores).
6. BRANCHES OF THE INTERNAL CAROTID ARTERY
Internal carotid artery(a. carotis interna) carries out the blood supply to the brain and organs of vision. The following parts are distinguished in it: cervical (pars cervicalis), stony (pars petrosa), cavernous (pars cavernosa) and cerebral (pars cerebralis). The cerebral part of the artery gives off the ophthalmic artery and divides into its terminal branches (anterior and middle cerebral arteries) at the inner edge of the anterior inclined process.
Branches of the ophthalmic artery(a. ophthalmica):
1) the central retinal artery (a. Centralis retinae);
2) the lacrimal artery (a. Lacrimalis);
3) posterior ethmoidal artery (a. Ethmoidalis posterior);
4) anterior ethmoidal artery (a. Ethmoidalis anterior);
5) long and short posterior ciliary arteries (aa. Ciliares posteriores longae et breves);
6) anterior ciliary arteries (aa. Ciliares anteriores);
7) muscle arteries (aa. Musculares);
8) the medial arteries of the eyelids (aa. Palpebrales mediales); anastomose with the lateral arteries of the eyelids, form the arch of the upper eyelid and the arch of the lower eyelid;
9) supra-block artery (a. Supratrochlearis);
10) dorsal artery of the nose (a. Dorsalis nasi).
V middle cerebral artery(a. cerebri media) distinguish between wedge-shaped (pars sphenoidalis) and insular parts (pars insularis), the latter continues into the cortical part (pars corticalis).
Anterior cerebral artery(a. cerebri anterior) connects to the opposite side of the artery of the same name by means of the anterior communicating artery (a. communicans anterior).
Posterior communicating artery(a. communicans posterior) is one of the anastomoses between the branches of the internal and external carotid arteries.
Anterior villous artery(a choroidea anterior).
7. BRANCHES OF THE CONNECTIVE ARTERY
In this artery, three sections are distinguished: the vertebral, internal thoracic arteries and the thyroid trunk depart from the first, the costal-cervical trunk from the second, and the non-permanent transverse neck artery from the third.
Branches of the first section:
1) vertebral artery(a. vertebralis), in which four parts are distinguished: prevertebral (pars prevertebralis), cervical (pars cervicalis), atlantic (pars atlantica) and intracranial (pars intracranialis).
Branches of the cervical part:
a) radicular branches (rr. radiculares);
b) muscle branches (rr. musculares).
Intracranial branches:
a) anterior spinal artery (a.spinalis anterior);
b) posterior spinal artery (a. spinalis posterior);
c) meningeal branches (rr. meningei) - front and back;
d) posterior lower cerebellar artery (a. inferior posterior cerebri).
The basilar artery (a.basilaris) is located in the groove of the bridge of the same name and gives the following branches:
a) labyrinth artery (a. labyrinthi);
b) middle cerebral arteries (aa. mesencephalicae);
c) the superior cerebellar artery (a. superior cerebelli);
d) anterior lower cerebellar artery (a. inferior anterior cerebelli);
e) bridge arteries (aa. pontis).
The right and left posterior cerebral arteries (aa. Cerebri posterior) close the arterial circle behind, the posterior communicating artery flows into the posterior cerebral artery, resulting in the formation of the arterial circle of the large brain (circulus arteriosus cerebri);
2) internal mammary artery(a. thoracica interna) gives:
a) bronchial and tracheal branches (rr. bronchiales et tracheales);
b) sternal branches (rr. sternales);
c) mediastinal branches (rr. mediastinales);
d) perforating branches (rr. perforantes);
e) thymic branches (rr. thymici);
f) pericardial diaphragmatic artery (a.pericardiacophrenica);
g) musculophrenic artery (a. musculophrenica);
h) the upper epigastric artery (a.epigastrica superior);
i) anterior intercostal branches (rr. intercostals anteriores);
3) shield-neck trunk(truncus thyrocervicalis) is divided into three branches:
a) lower thyroid artery (a. thyroidea inferior), giving tracheal branches (rr. tracheales), lower laryngeal artery (a. laryngealis inferior), pharyngeal and esophageal branches (rr. pharyngeales et oesophageales);
b) the suprascapular artery (a. suprascapularis), giving the acromial branch (r. acromialis);
c) the transverse neck artery (a. transversa cervicis), which is divided into superficial and deep branches.
Branches of the second section.
Costal-cervical trunk(truncus costocervicalis) is divided into deep cervical artery (a. cervicalis profunda) and the highest intercostal artery (a. intercostalis suprema).
Axillary artery(a. axillaris) is divided into three sections, is a continuation of the axillary artery.
Branches of the first section:
1) the upper thoracic artery (a.thoracica superior);
2) subscapular branches (rr. Subscapulares);
3) thoracoacromial artery (a. Thoracoacromialis); gives four branches: pectoral (rr. pectorales), subclavian (r. clavicularis), acromial (r. acromialis) and deltoid (r. deltoideus).
Branches of the second section:
1) lateral thoracic artery (a.thoracica lateralis). Gives the lateral branches of the mammary gland (rr. Mammarii lateralis).
Branches of the third section:
1) the anterior artery, the envelope of the humerus (a. Circumflexa anterior humeri);
2) the posterior artery, the envelope of the humerus (a. Circumflexa posterior humeri);
3) the subscapular artery (a. Subscapularis), dividing into the artery, the circumflex scapula (a. Circumflexa scapulae), and the thoracic artery (a. Thoracodorsalis).
8. SHOULDER ARTERY. ELBOW ARTERY. BRANCHES OF THE CHEST AORTE
Brachial artery(a. brachialis) is a continuation of the axillary artery, gives the following branches:
1) the upper ulnar collateral artery (a.collateralis ulnaris superior);
2) the lower ulnar collateral artery (a. Collateralis ulnaris inferior);
3) deep artery of the shoulder (a.profunda brachii), giving the following branches: middle collateral artery (a.collateralis media), radial collateral artery (a.collateralis radialis), deltoid branch (r. Deltoidei) and arteries feeding the humerus ( aa.nutriciae humeri).
Radial artery(a. radialis) is one of the two terminal branches of the brachial artery. The terminal section of this artery forms a deep palmar arch (arcus palmaris profundus), anastomosing with the deep palmar branch of the ulnar artery. Branches of the radial artery:
1) superficial palmar branch (r. Palmaris superficialis);
2) radial recurrent artery (a. Reccurens radialis);
3) dorsal carpal branch (r. Carpalis dorsalis); participates in the formation of the dorsal network of the wrist (rete carpale dorsale);
4) palmar carpal branch (r. Carpalis palmaris).
Ulnar artery(a. ulnaris) is the second terminal branch of the brachial artery. The terminal section of this artery forms a superficial palmar arch (arcus palmaris supreficialis), anastomosing with the superficial palmar branch of the radial artery. Branches of the ulnar artery:
2) muscle branches (rr. Musculares);
3) the common interosseous artery (a. Interuossea communis), dividing into the anterior and posterior interosseous arteries;
4) deep palmar branch (r. Palmaris profundus);
5) palmar carpal branch (r. Carpalis palmaris).
There are many anastomoses in the subclavian, axillary, brachial, ulnar and radial arteries system, due to which the blood supply to the joints and collateral blood flow are provided.
The branches of the thoracic aorta are subdivided into visceral and parietal.
Visceral branches:
1) pericardial branches (rr. Pericardiaci);
2) esophageal branches (rr. Oesophageales);
3) mediastinal branches (rr. Mediastinaes);
4) bronchial branches (rr. Bronchiales).
Parietal branches:
1) the superior phrenic artery (a.phrenica superior);
2) posterior intercostal arteries (aa. Intercostales posteriores), each of which gives off a medial cutaneous branch (r. Cutaneus medialis), a lateral cutaneous branch (r. Cutaneus lateralis) and a dorsal branch (r. Dorsalis).
9. BRANCHES OF THE ABDOMINAL AORTE
The branches of the abdominal part of the aorta are subdivided into visceral and parietal.
Visceral branches, in turn, are divided into paired and unpaired.
Paired visceral branches:
1) ovarian (testicular) artery (a. Ovarica (a testicularis). The ovarian artery gives tube (rr. Tubarii) and ureteral branches (rr. Ureterici), and the testicular artery - the epididymis (rr. Epididymales) and ureteral branches (rr. ureterici);
2) renal artery (a. Renalis); gives the ureteral branches (rr. ureterici) and the lower adrenal artery (a. suprarenalis inferior);
3) the middle adrenal artery (a. Suprarenalis media); anastomoses with the superior and inferior adrenal arteries.
Unpaired visceral branches:
1) celiac trunk (truncus coeliacus). It is divided into three arteries:
a) splenic artery (a. lienalis), gives branches to the pancreas (rr. pancreatici), short gastric arteries (aa. gastricae breves) and the left gastroepiploic artery (a. gastroepiploica sinistra), giving omental and gastric branches;
b) common hepatic artery (a. hepatica communis); divided into its own hepatic artery (a. hepatica propria) and gastroduodenal artery (a. gastroduodenalis). The own hepatic artery gives off the right gastric artery (a. Gastrica dextra), the right and left branches, the gallbladder artery (a. Cystica) departs from the right branch. The gastroduodenal artery is divided into the upper pancreatoduodenal arteries (aa. Pancreaticoduodenales superiores) and the right gastroepiploic artery (a. Gastroepiploica).
c) the left gastric artery (a. gastrica sinistra), gives off the esophageal branches (rr. oesophagealis);
2) the superior mesenteric artery (a. Mesenterica superior). Gives the following branches:
a) the right colic artery (a. colica dextra); anastomoses with the branches of the middle colon artery, the branch of the ilio-colon artery;
b) the middle colic artery (a. colica media); anastomoses with the right and left colonic arteries;
c) the ilio-colonic artery (a. ileocolica); gives an artery of the appendix (a. appendicularis), a colon-intestinal branch (r. colicus), anterior and posterior cecum arteries (aa. caecalis anterior et posterior);
d) lower pancreatoduodenal arteries (aa. pancreaticoduodenalies inferiors);
e) ileal-intestinal (aa. ileales) and jejunal arteries (aa. jejunales);
3) the lower mesenteric artery (a. Mesenterica inferior). Gives the following branches:
a) sigmoid arteries (aa.sigmoidei);
b) the left colic artery (a. colica sinistra);
c) the superior rectal artery (a. rectalis superior).
Parietal branches:
1) four pairs of lumbar arteries (aa. Lumbales), each of which gives off the dorsal and spinal branches;
2) the lower phrenic artery (a. Phrenica inferior), giving the upper adrenal arteries (aa. Suprarenales superiores).
At the level of the middle of the body of the IV lumbar vertebra, the abdominal part of the aorta is divided into two common iliac arteries, and itself continues into the median sacral artery (a.sacralis mediana).
10. STRUCTURE OF THE BRANCHES OF THE COMMON LIQUID ARTERY
Common iliac artery(a. iliaca communis) is divided into the internal and external iliac arteries at the level of the ilio-sacral articulation.
External iliac artery(a. iliaca externa) gives the following branches:
1) deep artery, circumflex iliac bone (a. Circumflexa iliaca profunda);
2) the lower epigastric artery (a. Epigastrica inferior), giving the pubic branch (r. Pubicus), the cremasteric artery (a. Cremasterica) in men and the artery of the round ligament of the uterus (a. Lig teretis uteri) in women.
Internal iliac artery(a. iliaca interna) gives the following branches:
1) the umbilical artery (a. Umbilicalis), presented in an adult by the medial umbilical ligament;
2) the superior gluteal artery (a. Glutealis superior), which is divided into deep and superficial branches;
3) the lower gluteal artery (a. Glutealis inferior); gives the artery accompanying sciatic nerve(a. comitans nervi ischiadici);
4) the ilio-lumbar artery (a. Iliolumbalis), giving the iliac (r. Iliacus) and lumbar branches (r. Lumbalis);
5) the uterine artery (a. Uterine), giving the tube (r. Tubarius), ovarian (r. Ovaricus) and vaginal branches (rr. Vaginales);
6) the lower urinary artery (a. Vesicalis inferior);
7) lateral sacral arteries (aa.sacrales laterales), giving off the spinal branches (rr.spinales);
8) internal genital artery (a. Pudenda interna); gives the lower rectal artery (a. rectalis inferior) and in women: urethral artery (a. urethralis), dorsal and deep arteries of the clitoris (aa. dorsalis et profunda clitoritidis) and artery of the vestibule bulb (a. bulbi vestibule); in men: urethral artery (a. urethralis), dorsal and deep arteries of the penis (aa. dorsalis et profunda penis), artery of the bulb of the penis (a. bulbi penis);
9) the middle rectal artery (a. Rectalis media);
10) obturator artery (a. Obturatoria); divided into anterior and posterior branches. The latter gives off the acetabular branch (r. Acetabularis). The obturator artery in the pelvic cavity gives off the pubic branch (r. Pubicus).
11. BRANCHES OF THE FEMORAL, PENDANT, ANTERIOR AND PREVIOUS TIBOUS ARTERIES
Femoral artery(a. femoralis) is a continuation of the external iliac artery and gives the following branches:
1) deep artery of the thigh (a. Profunda femoris), giving perforating arteries (aa. Perforantes); the lateral artery, bending around the femur (a. circumflexa femoris lateralis), giving the ascending, transverse and descending branches (rr. ascendens, transversus et descendens); the medial artery, the circumflex of the femur (a.circumflexa femoris medialis), giving the acetabular branch (r. acetabularis) to hip joint, deep and ascending branches (rr.profundus et ascendens);
2) the superficial artery, the circumflex of the ilium (a. Circumflexa iliaca superficialis);
3) superficial epigastric artery (a. Epigastrica superficialis);
4) the descending knee artery (a. Genus descendens); participates in the formation of the knee articular network (rete articulare genus);
5) external genital arteries (aa. Pudendae externae).
Popliteal artery(a. poplitea) is a continuation of the femoral and gives the following branches:
1) the medial lower knee artery (a. Genus inferior medialis); participates in the formation of the knee articular network (rete articulare genus);
2) the lateral lower knee artery (a. Genus inferior lateralis);
3) the medial superior knee artery (a. Genus superior medialis);
4) the lateral superior knee artery (a. Genus superior lateralis);
5) the middle knee artery (a. Genus media).
Anterior tibial artery(ayu tibialis anterior) departs from the popliteal artery in the popliteal fossa and gives the following branches:
1) anterior tibial recurrent artery (a.reccurens tibialis anterior);
2) the posterior tibial recurrent artery (a. Reccurens tibialis posterior);
3) the medial anterior ankle artery (a. Malleolaris anterior medialis);
4) lateral anterior ankle artery (a. Malleolaris anterior lateralis);
5) muscle branches (rr. Musculares);
6) dorsal artery of the foot (a.dorsalis pedis); gives the lateral and medial tarsal arteries (aa.tarsales lateralis et medialis), the arcuate artery (a.arcuata) and is divided into terminal branches: the deep plantar artery (a.plantaris profunda) and the first dorsal metatarsal artery (.a metatarsalis dorsalis I).
Posterior tibial artery(a. tibialis posterior) is a continuation of the popliteal artery and gives the following branches:
1) the medial plantar artery (a. Plantaris medialis), dividing into deep and superficial branches;
2) lateral plantar artery (a. Plantaris lateralis); forms a deep plantar arch (arcus plantaris profundus), from which four plantar metatarsal arteries (aa.metatarsales plantares I-IV) depart. Each metatarsal artery passes into the common plantar digital artery (a. Digitalis plantaris communis), which (except for I) are divided into two own plantar digital arteries (aa. Digitalis plantaris propriae);
3) a branch enveloping the fibula (r. Circumflexus fibularis);
4) peroneal artery (a. Peronea);
5) muscle branches (rr. Musculares).
12. SYSTEM OF UPPER CAVITY VIENNA
Superior vena cava(v. cava superior) collects blood from the veins of the head, neck, both upper limbs, veins of the thoracic and partially abdominal cavities and flows into the right atrium. The azygos vein flows into the superior vena cava on the right, and the mediastinal and pericardial veins on the left. It has no valves.
Unpaired Vienna (v. Azygos) is a continuation into the chest cavity of the right ascending lumbar vein (v. lumbalis ascendens dextra), has two valves in the mouth. The unpaired vein, esophageal veins, mediastinal and pericardial veins, posterior intercostal veins IV-XI and the right superior intercostal veins flow into the azygos vein.
Semi-unpaired vein(v. hemiazygos) is a continuation of the left ascending lumbar vein (v. lumbalis ascendens sinistra). The mediastinal and esophageal veins, an accessory semi-unpaired vein (v. Hemiazygos accessoria), which takes the I-VII upper intercostal veins, the posterior intercostal veins, flow into the semi-unpaired vein.
Posterior intercostal veins(vv. intercostales posteriores) collect blood from the tissues of the walls of the chest cavity and part of the abdominal wall. The intervertebral vein (v. Intervertebralis) flows into each posterior intercostal vein, into which, in turn, the spinal branches (rr. Spinales) and the back vein (v. Dorsalis) flow.
The veins of the spongy substance of the vertebrae and spinal veins flow into the internal anterior and posterior vertebral venous plexuses (plexus venosi vertebrales interni). Blood from these plexuses flows into the accessory semi-unpaired and azygos veins, as well as into the external anterior and posterior vertebral venous plexuses (plexus venosi vertebrales externi), from which blood flows into the lumbar, sacral and intercostal veins and into the accessory semi-unpaired and azygos veins.
Right and left brachiocephalic veins(vv. brachiocephalicae dextra et sinistra) are the roots of the superior vena cava. They have no valves. Collect blood from the upper extremities, organs of the head and neck, upper intercostal spaces. The brachiocephalic veins form when the internal jugular and subclavian veins merge.
Deep cervical vein(v. cervicalis profunda) originates from the external vertebral plexuses and collects blood from the muscles and the auxiliary apparatus of the muscles of the occipital region.
Vertebral vein(v vertebralis) accompanies the artery of the same name, taking blood from the internal vertebral plexuses.
Internal thoracic vein(v. thoracica interna) accompanies the artery of the same name on each side. The anterior intercostal veins (vv. Intercostales anteriores) flow into it, and the roots of the internal thoracic vein are the musculophrenic vein (v. Musculophrenica) and the upper epigastric vein (v. Epigastrica superior).
13. VENINS OF THE HEAD AND NECK
Internal jugular vein(v. jugularis interna) is a continuation of the sigmoid sinus of the hard shell of the brain, has an upper bulb in the initial section (bulbus superior); above the confluence with the subclavian vein is the lower bulb (bulbus inferior). There is one valve above and below the lower bulb. Intracranial tributaries of the internal jugular vein are the eye veins (vv. Ophthalmicae superior et inferior), the veins of the labyrinth (vv. Labyrinthi) and diploic veins.
Through the diploic veins(vv. diploicae): posterior temporal diploic vein (v. diploica temporalis posterior), anterior temporal diploic vein (v. diploica temporalis anterior), frontal diploic vein (v. diploica) and occipital diploic vein (v. diploica occipitalis) - blood flows from the bones of the skull; have no valves. With the help of the emissary veins (vv. Emissariae): the mastoid emissary vein (v. Emissaria mastoidea), the condylar emissary vein (v. Emissaria condylaris) and the parietal emissary vein (v emissaria parietalis) - the diploic veins communicate with the veins of the outer covers of the head.
Extracranial tributaries of the internal jugular vein:
1) the lingual vein (v. Lingualis), which is formed by the deep vein of the tongue, the hyoid vein, the dorsal veins of the tongue;
2) facial vein (v. Facialis);
3) the upper thyroid vein (v. Thyroidea superior); has valves;
4) pharyngeal veins (vv. Pharyngeales);
5) submandibular vein (v. Retromandibularis).
External jugular vein(v. jugularis externa) has paired valves at the level of the mouth and middle of the neck. The transverse veins of the neck (vv. Transversae colli), the anterior jugular vein (v. Jugularis anterior), and the suprascapular vein (v. Suprascapularis) flow into this vein.
Subclavian vein(v. subclavia) unpaired, is a continuation of the axillary vein.
14. THE VEINS OF THE UPPER LIMB. LOWER CAVITY VIENNA SYSTEM. GATE VENA SYSTEM
These veins are represented by deep and superficial veins.
The palmar digital veins fall into the superficial palmar venous arch (arcus venosus palmaris superficialis).
Paired palmar metacarpal veins flow into the deep palmar venous arch (arcus venosus palmaris profundus). Superficial and deep venous arches continue into paired radial and ulnar veins (vv. Radiales et vv palmares), which belong to the deep veins of the forearm. From these veins, two brachial veins (vv. Brachiales) are formed, which merge and form an axillary vein (v. Axillaries), which passes into the subclavian vein.
Superficial veins of the upper limb.
Dorsal metacarpal veins together with their anastomoses form the dorsal venous network of the hand (rete venosum dorsale manus). The superficial veins of the forearm form a plexus in which the lateral saphenous vein of the hand (v. Cephalica), which is a continuation of the first dorsal metacarpal vein, and the medial saphenous vein of the hand (v. Basilica), which is a continuation of the fourth dorsal metacarpal vein, are isolated. The lateral saphenous vein flows into the axillary vein, and the medial one into one of the brachial veins. Sometimes there is an intermediate vein of the forearm (v. Intermedia antebrachii). The intermediate vein of the elbow (v. Intermedia cubiti) is located in the anterior elbow region (under the skin), has no valves.
There are parietal and visceral tributaries of the inferior vena cava (v. Cava inferior).
Visceral tributaries:
1) renal vein (v. Renalis);
2) adrenal vein (v. Suprarenalis); has no valves;
3) hepatic veins (vv. Hepaticae);
4) ovarian (testicular) vein (v. Ovarica (testicularis)).
Parietal tributaries:
1) lower phrenic veins (vv. Phrenicae inferiors);
2) lumbar veins (vv. Lumbales).
Portal vein(v. portae) is the largest visceral vein, its main tributaries are the splenic vein, superior and inferior mesenteric veins.
Splenic vein(v. lienalis) merges with the superior mesenteric vein and has the following tributaries: the left gastroepiploic vein (v. gastroepiploica sinistra), short gastric veins (vv. gastricae breves) and pancreatic veins (vv. pancreaticae).
Superior mesenteric vein(v. mesenterica superior) has the following tributaries: the right gastroepiploic vein (v. gastroepiploica dextra), the ilio-colon vein (v. ileocolica), the right and middle colic veins (vv. colicae media et dextra), pancreatic veins (vv . pancreaticae), a vein of the appendix (v. appendicularis), veins of the ileum and jejunum (vv. ileales et jejunales).
Inferior mesenteric vein(v. mesenterica inferior) flows into the splenic vein, is formed when the sigmoid veins (vv. sigmoideae), the superior rectal vein (v. rectalis superior) and the left colon vein (v. colica sinistra) merge.
Before entering the gate of the liver, the right and left gastric veins (vv. Gastricae dextra et sinistra), the pre-pyloric vein (v. Prepylorica) and the biliary vein (v. Cystica) flow into the portal vein. Entering the gates of the liver, the portal vein is divided into right and left branches, which in turn are divided into segmental, then into interlobular veins, which extend sinusoidal vessels into the lobules and flow into the central vein. Sublobular veins emerge from the lobules, which merge and form the hepatic veins (vv. Hepaticae).
15. VENINS OF THE PELVIS AND LOWER LIMBS
The right and left common iliac veins (vv. Iliacae communes) form the inferior vena cava.
External iliac vein(v. iliaca externa) unites with the internal iliac vein at the level of the sacroiliac joint and forms the common iliac vein. The external iliac vein receives blood from all veins of the lower limb; has no valves.
The internal iliac vein has visceral and parietal tributaries.
Visceral tributaries:
1) vaginal venous plexus (plexus venosus vaginalis), passing into the uterine venous plexus (plexus venosus uterinus);
2) the prostate venous plexus (plexus venosus prostaticus);
3) urinary venous plexus (plexus venosus vesicalis);
4) rectal venous plexus (plexus venosus rectalis);
5) sacral venous plexus (plexus venosus sacralis).
Parietal tributaries:
1) ilio-lumbar vein (v. Ilicolumbalis);
2) upper and lower gluteal veins (vv. Glutealis superiores et inferiors);
3) lateral sacral veins (vv. Sacrales laterales);
4) obturator veins (vv. Obturatoriae).
Deep veins of the lower limb:
1) femoral vein (v. Femoralis);
2) deep vein of the thigh (v. Femoris profunda);
3) popliteal vein (v. Poplitea);
4) anterior and posterior tibial veins (vv. Tibiales anteriores et posteriores);
5) peroneal veins (vv. Fibulares).
All deep veins (except for the deep vein of the thigh) accompany the arteries of the same name; have many valves.
Superficial veins of the lower extremity:
1) great saphenous vein of the leg (v. Saphena magna); flows into the femoral vein, has many valves. Collects blood from the soles of the feet, anteromedial surface of the lower leg and thigh;
2) small saphenous vein of the leg (v. Saphena parva); flows into the popliteal vein, has many valves. Collects blood from the lateral part of the foot, heel region, saphenous veins of the sole and dorsal venous arch;
3) plantar venous arch (arcus venosus plantares); collects blood from the plantar digital veins; from the arch, blood flows into the posterior tibial veins along the plantar veins (lateral and medial);
4) dorsal venous arch (arcus venosus dorsalis pedis); collects blood from the dorsal digital veins; from the arch the blood flows into the greater and lesser saphenous veins.
There are numerous anastomoses between the systems of the superior and inferior vena cava and the portal vein.
The cardiovascular system and its brief characteristics
The existence of all highly developed animals and humans is based on the cardiovascular system. It carries out the interconnection of all parts of the body, providing metabolism. All this imposes certain requirements on the system. Thanks to vessels of various calibers, interconnection with all parts of the body is ensured. The liquid consistency of blood facilitates the rapid movement of substances. This means that the speed of their exchange is acceptable. The structure of the heart muscle allows the organ to work continuously throughout life.
The structure of the cardiovascular system
The cardiovascular system in all animals (which have it) and in humans consists of 2 sections.
1. Bearing component. Provides the movement of substances throughout the body. In this case, it is blood.
2. Pumping element. It provides the movement of blood. In highly developed animals and humans, this organ is called the heart.
3. Backbone component. Provides direction of travel. They are vessels.
Brief characteristics of the human cardiovascular system
In general terms, the human cardiovascular system can be represented as follows.
1. The central organ is the heart, which is divided lengthwise into two halves. Each of which is divided into two sections. One ventricle and one atrium. Between them there is a hole with valves that provide one-way blood flow. Thus, a four-chambered organ is obtained. In it, the right sections (ventricle and atrium) do not have communication with the left chambers, so that blood of two different types does not mix. One oxygen-depleted.  It is called venous. In the other, the amount of oxygen is much higher. This is arterial blood. Venous blood passes through the right chambers of the heart and they are responsible for its movement. Arterial blood passes through the left sections.
It is called venous. In the other, the amount of oxygen is much higher. This is arterial blood. Venous blood passes through the right chambers of the heart and they are responsible for its movement. Arterial blood passes through the left sections.
2. Blood vessels. They are grouped into two circles of blood circulation. The so-called pulmonary circulation consists of the vessels of the lungs. It carries out gas exchange. Carbon dioxide enters the lungs from the blood, and it is saturated with atomic oxygen. The systemic circulation takes an active part in the metabolism (including oxygen and carbon dioxide) throughout the body.
Insufficiency of the circulatory system
Naturally, the cardiovascular system, which supplies blood to the entire body, is considered the most important. Therefore, if its work is disrupted, all other organs suffer. Chronic cardiovascular insufficiency deserves special attention as one of the main causes of disability among the population. It may be based on vascular or heart pathology.
Causes of insufficiency of the circulatory system
All causes that can lead to a malfunction of the system can be divided into 3 groups: cardiac (cardiac), vascular and mixed.
1. Cardiac causes take the leading place in terms of quantity. First of all, such statistics are associated with the fact that the cardiovascular system directly depends on the work of its main organ - the heart.  These reasons include myocardial infarction, endocarditis, pericarditis, myocarditis, coronary heart disease, various types of cardiomyopathy, and others.
These reasons include myocardial infarction, endocarditis, pericarditis, myocarditis, coronary heart disease, various types of cardiomyopathy, and others.
2. Vascular causes. At the beginning of their development, they do not affect the work of the heart, for example, varicose veins of the lower extremities or hemorrhoids.
3. Mixed causes affect the entire system, including the heart itself (more precisely, its vessels - coronary arteries). This is, for example, atherosclerosis.